
 President Jimmy Carter’s cancer remission was wonderful news, but as some outlets [1] noted, it is important to understand that not all patients are responding as well to similar treatments, and that there is currently still no “cure” for cancer. However, President Carter’s remission has brought more attention and research into new antibody based drugs targeting immune checkpoints.
President Jimmy Carter’s cancer remission was wonderful news, but as some outlets [1] noted, it is important to understand that not all patients are responding as well to similar treatments, and that there is currently still no “cure” for cancer. However, President Carter’s remission has brought more attention and research into new antibody based drugs targeting immune checkpoints.
(View ProSci’s range of cancer products here)
Immune checkpoints: PD-1 antibodies from ProSci
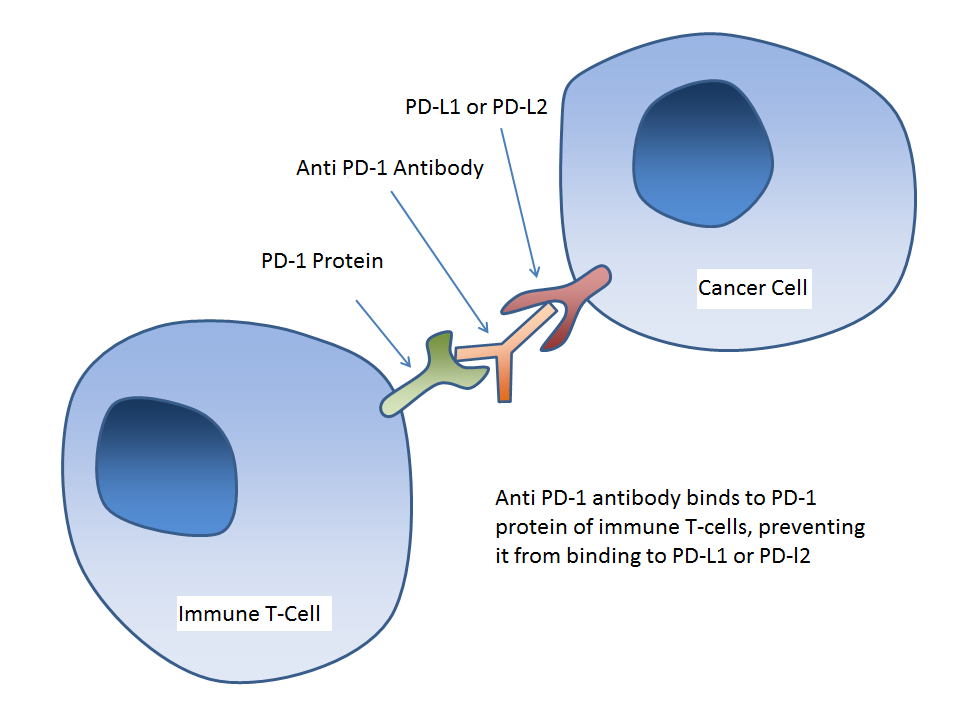
Immune checkpoints are molecules that provide signals to the immune system, telling it whether an object or cell is safe and should be left alone, or if it is foreign and should be attacked. It has now been discovered that cancers evade the immune system through interaction with these checkpoints. The antibody drug prescribed to President Carter, pembrolizumab (Keytruda®), is a monoclonal antibody that targets PD-1 (Programmed Death 1), an immune checkpoint protein found on cytotoxic T-cells. Cancer cells over-express the PD-1 ligands, PD-L1 or PD-L2, which provide a negative signal to T-cells that prevent their activation, and suppress the body’s immune response against cancer. Monoclonal antibodies such as pembrolizumab can block these incoming signals from cancer cells, allowing them to be “seen” by the immune system and targeted for lysis. This form of treatment, in which an antibody is used to target a protein involved in the immune checkpoint process to elicit a desired immune response is called an immunotherapy.
Immunotherapy
Immunotherapy is one of the newest facets of cancer treatment, and has taken the antibody industry by storm. Going hand in hand with the concept of personalized medicine tailored to a patient’s own genome, immunotherapy has the scientific community bustling with new research activity. The two current PD-1 drugs on the market are nivolumab (Opdivo®)[2], a fully human monoclonal antibody, and pembrolizumab (Keytruda®)[3], a humanized mouse monoclonal antibody. Nivolumab and pembrolizumab express an overall response rate of 32% and 34% respectively in the case of melanoma treatment, where a response is any form of tumor growth regulation or shrinkage.[4] To improve upon these numbers, the research community is turning toward combination immunotherapy, in which immunogenic pharmaceuticals like these PD-1 antibodies would be used in conjunction with other methods of treatment like chemotherapy, or even other forms of immunotherapy.[5]
Learn more about immunotherapy here
Potential risks with immunotherapy: PD-1 and CTLA-4
 As with any new medicine, there are potential risks with immunotherapy. The goal of immunotherapy is to modify T-cell activity through either activating or deactivating pathways which allows immunocytes to seek desired targets. PD-1 monoclonal antibodies boost the immune system by blocking the part of PD-1 where PD-L1 (or PD-L2) would bind, preventing the negative signal from being transmitted, and preventing the deactivation of the T-cells. But by blocking the negative signal proteins on killer T-cells which are normally helpful in tolerance to self, it is possible that they would attack not only cancer cells, but other non-cancerous cells as well. PD-1 itself has proven to be relatively safe, with toxicity rates reported between 12-13% of patients reaching grade 3-4 adverse effects. Patients were also receiving chemotherapy and dacarbazine, leaving them more susceptible to a reaction.[6] However, Kobold et. al also shows some more concerning rates of toxicity: patients receiving ipilimumab (Yervoy®)[7], an antibody that targets the CTLA-4 protein of immune T-cells, showed grade 3-4 adverse effects in 50% of cases. Patients receiving blinatumomab (Blincyto®)[8], a bispecific antibody that helps to bring killer T-cells and cancerous B-cells together to assist with activation of the immune system, showed grade 3, 4, and 5 adverse effects in 83% of patients receiving this treatment. These other immunotherapies are showing rates of more frequent, and more severe adverse reactions overall, which is concerning. If combination immunotherapy is to succeed, more research into how to regulate the immune system without adverse effects will need to be investigated. This will assure at least some quality of life for the patient as Kobold wrote.
As with any new medicine, there are potential risks with immunotherapy. The goal of immunotherapy is to modify T-cell activity through either activating or deactivating pathways which allows immunocytes to seek desired targets. PD-1 monoclonal antibodies boost the immune system by blocking the part of PD-1 where PD-L1 (or PD-L2) would bind, preventing the negative signal from being transmitted, and preventing the deactivation of the T-cells. But by blocking the negative signal proteins on killer T-cells which are normally helpful in tolerance to self, it is possible that they would attack not only cancer cells, but other non-cancerous cells as well. PD-1 itself has proven to be relatively safe, with toxicity rates reported between 12-13% of patients reaching grade 3-4 adverse effects. Patients were also receiving chemotherapy and dacarbazine, leaving them more susceptible to a reaction.[6] However, Kobold et. al also shows some more concerning rates of toxicity: patients receiving ipilimumab (Yervoy®)[7], an antibody that targets the CTLA-4 protein of immune T-cells, showed grade 3-4 adverse effects in 50% of cases. Patients receiving blinatumomab (Blincyto®)[8], a bispecific antibody that helps to bring killer T-cells and cancerous B-cells together to assist with activation of the immune system, showed grade 3, 4, and 5 adverse effects in 83% of patients receiving this treatment. These other immunotherapies are showing rates of more frequent, and more severe adverse reactions overall, which is concerning. If combination immunotherapy is to succeed, more research into how to regulate the immune system without adverse effects will need to be investigated. This will assure at least some quality of life for the patient as Kobold wrote.
Further Studies
These risks of immunotherapy can definitely be avoided through greater understanding of the mutations we see in different cancers. Rizvi et. al [9] is an excellent example, showing a correlation between the number of mutations in non-small cell lung cancers (NSCLC) correlated to the effectiveness of anti PD-1 antibodies. The study showed that PD-1 antibodies (pembrolizumab) were more effective against cancers displaying “molecular smoking signature, higher neoantigen burden, and DNA repair pathway mutations,” and showing an increased level of shrinkage and growth regulation. Cancer cells can only display so many immune checkpoint proteins. Every time an antibody is introduced to block an immune pathway that the cancer is displaying, it increases the chance a T-cell will recognize the caner as a target; however, introducing antibodies that target T-cells and boost the immune system could increase the chances of the immunocyte targeting cells that use the same immune checkpoint pathway as the cancer. Every time an antibody introduced against a T-cell receptor, it increases the number of liable targets. Research like Rizvi’s shows the importance of working toward precision therapies, in which the best possible group of medicines can be administered based on the genetic makeup of a cancerous cell.
The landscape of immunotherapy is changing quickly. The recent success stories have us not questioning whether this strategy can work, but instead how to make it better, and how to do it safely. At ProSci, we have completed the development of single domain antibodies against the PD-1 receptor, and are in the process of developing single domain antibodies against PD-L1 as well. These llama single domain antibodies (sdab) hold special characteristics which make them amenable to possible therapeutics. ProSci are looking to form a partnership with those who are willing to help characterize these antibodies for functionality. If you’re interested, please contact us.
Find out how ProSci can help your Antibody needs today!
References
1: DeMonaco, Harold J. “What the Media Got Wrong about Jimmy Carter’s Cancer
“Cure”” HealthNewsRevieworg. N.p., n.d. Web. 12 Feb. 2016.
2, 3: “NCI Drug Dictionary.” National Cancer Institue. N. p., n.d. Web. 12 Feb. 2016
4: Ascierto, Paolo A., and Francesco M. Marincola. “2015: The Year of Anti-PD-1/PD-L1s Against
Melanoma and Beyond.” EBioMedicine 2.2 (2015): 92-93. Web.
5: Cavallo, Jo, and Robert H. Pierce. “Determining Why Not All Patients Respond to PD-1 Inhibitors.” The
ASCO Post. N.p., n.d. Web. 12 Feb. 2016.
6: Kobold, S. “Immunotherapy in Tumors (27.11.2015).” Deutsches Ärzteblatt:. N.p., n.d. Web. 12 Feb. 2016.
7, 8: “NCI Drug Dictionary.” National Cancer Institute. N.p., n.d. Web. 12 Feb. 2016.
9: Rizvi, Nayier A. “Mutational Landscape Determines Sensitivity to PD-1 Blockade in Non–small Cell Lung
Cancer.” ScienceMag.org. Science Magazine, 3 Apr. 2015. Web. 12 Feb. 2016.
Questions? Get in touch.
Originally posted by Prosci Inc.
![]()